
 Little League® guidelines may not be strict enough to prevent injuries
Little League® guidelines may not be strict enough to prevent injuries
Sinding-Larsen-Johansson syndrome is characterized by a stress injury to the growing patella (kneecap) at its inferior pole (bottom) where the patellar tendon attaches and experiences large forces from the powerful quadriceps (thigh) muscles. This aspect of this growing patella bone is an area of relative weakness and injury to it occurs from repetitive stress during vigorous exercise and activity. This is the site of origin of the patellar tendon. There is traction on the patella at this point due to action of the large, powerful thigh muscle (quadriceps), as well as with deep bending of the knee. It is usually a temporary condition that is uncommon after age 16 or when the growth is completed. It is the children’s equivalent of patellar tendinitis (jumper’s knee).
Sinding-Larsen-Johansson Syndrome results from stress (a single sudden incident or repeated) or injury of the lower patella that overstresses the developing bone, causing pain. This may be inflammation of the cartilage of the growing patella, death of tendon cells from repeated stress, or pulling off the lining of the patellar bone.
Initial treatment consists of medications and ice to relieve pain, stretching and strengthening exercises, and modification of activities. Specifically, kneeling, jumping, squatting, stair climbing, and running on the affected knee should be avoided. The exercises can all be carried out at home for acute cases. Chronic cases often require a referral to a physical therapist or athletic trainer for further evaluation or treatment. Uncommonly, the affected leg may be temporarily immobilized if symptoms are severe. A patellar band (brace between the kneecap and tibial tubercle on top of the patellar tendon) may help relieve symptoms. Rarely, surgery is needed (if conservative treatment fails) in the growing patient. In addition, surgery may be necessary after skeletal maturity if the ossicle becomes painful.
Learn More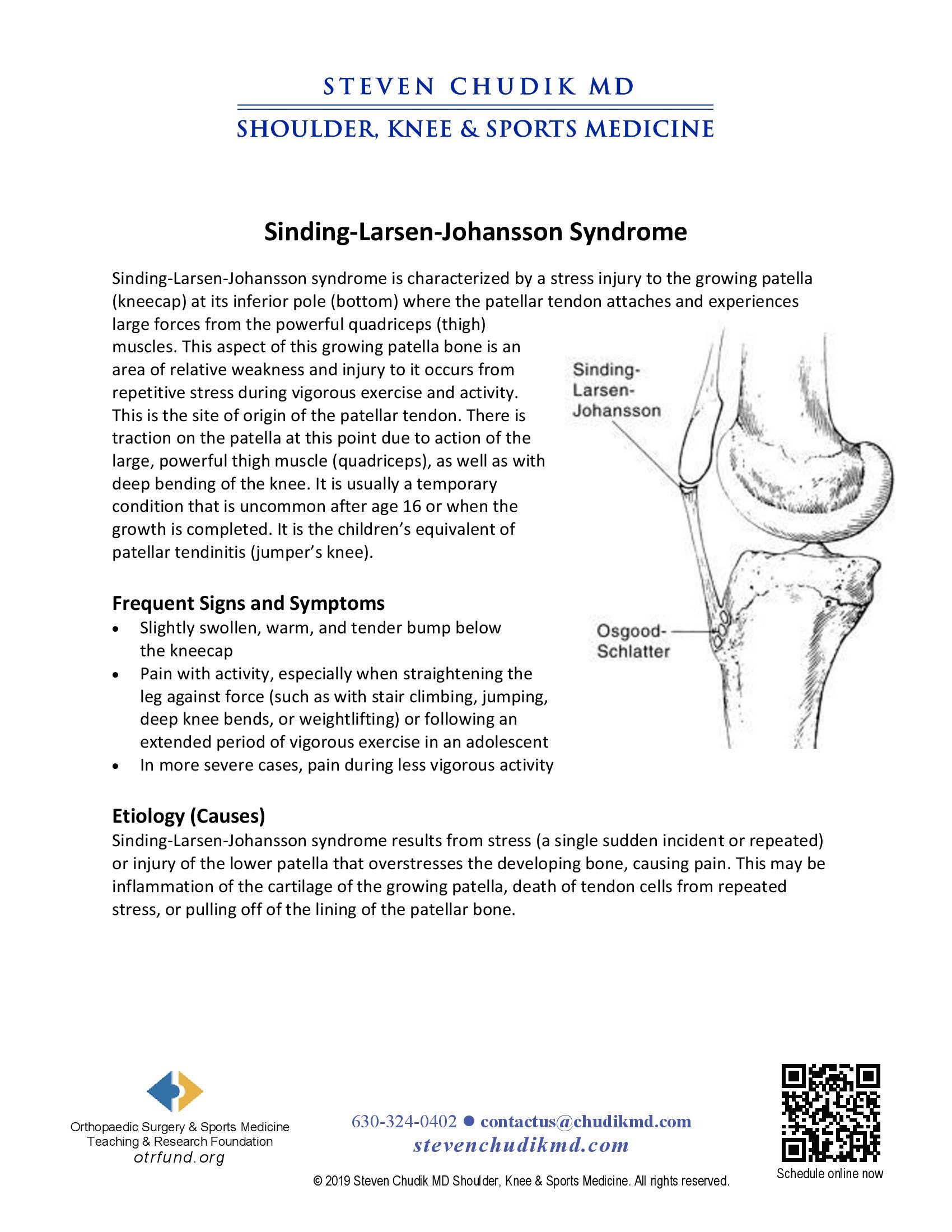
 A race against time: Frantz’s passion versus prudence
A race against time: Frantz’s passion versus prudence
Dr Steven Chudik founded OTRF in 2007 to keep people active and healthy through unbiased education and research. Click to learn about OTRF’s free programs, educational opportunities and ways to participate with the nonprofit foundation.
4700 Gilbert Ave, Suite 51
Western Springs, Illinois 60558
Phone: 630-324-0402
Fax: 630-920-2382

© 2026 © 2019 Copyright Steven Chudik MD, All Rights Reserved.



